ABDOMINAL PELVIC TRAUMA. Dr. Burkan Nasr Consultant Surgeon Advanced Laparoscopic, Bariatric, GI And Hernia Surgeon.
|
|
|
- Burkan Nasr
- 11 days ago
- Views:
Transcription
1 ABDOMINAL PELVIC TRAUMA Dr. Burkan Nasr Consultant Surgeon Advanced Laparoscopic, Bariatric, GI And Hernia Surgeon.


2 OBJECTIVE - ANATOMY - CLASSIFICATION - SOLID ORGAN INJURY - HOLLOW ORGAN INJURY - RETROPERITONEAL HEMATOMA - Renal and Urinary tract injury - Pelvic injury

3 ANATOMY
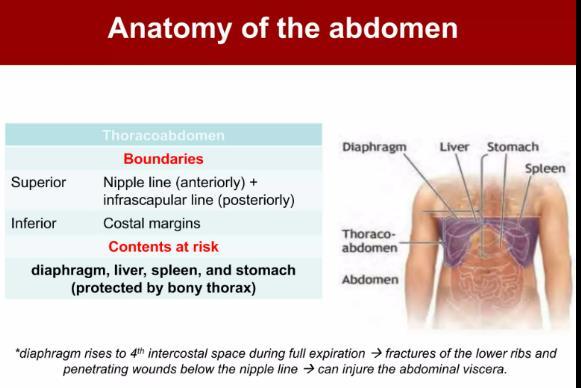
4 Regions of the abdomen peritoneal cavity subdivided into: Thoraco-Abdomen segment: covered by bony thorax and includes diaphragm, liver, spleen. Abdominal segment: stomach, Small bowel and transverse colon Retroperitoneum: aorta, vena cava, pancreas, kidneys, ureters and portions of duodenum and colon (injuries to this region notoriously difficult to diagnose because the area is remote from physical examination and is not sampled by peritoneal lavage) Pelvic organs: rectum, bladder, iliac vessels, internal genitalia of women (injury also difficult to diagnose early because of anatomical location )

5
6

7

8

9
10 Types of Abdominal trauma ; Blunt Trauma Penetrating Trauma
11 BLUNT TRAUMA: A force to the abdomen that does not leave an open wound The spleen and liver the most frequently injured organs, Small and large intestines are the next most injured organs Etiology -Road traffic accident -Falls from height -During sporting activity -Industrial accident
.")
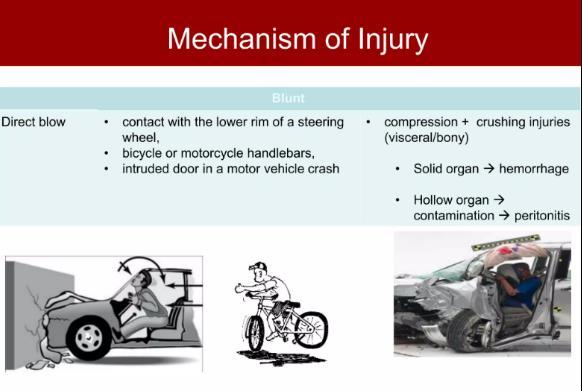
12 Mechanisms of injury two primary mechanisms of injury compression forces and deceleration forces. Compression forces: may result from direct blows or external compression against a fixed object (spinal column). Deceleration forces: cause stretching and linear shearing between relatively fixed and free objects.

13

14


15
16 What is the seat belt sign? Bruises or abrasions on the anterior abdominal wall due to the restraint of a seat belt. It often indicates an underlying visceral injury duodenal transection, mesenteric hematomas, retroperitoneal injuries and lumbar spine fractures (chance fractures). What are the possible injuries abdomen hits by the handle bars of bike or motor cycle? Transection of the duodenum Duodenal hematoma Pancreatic trauma
17 How do you approach of pt. with blunt trauma?? 1- history 2- physical examination 3- investigation 4- treatment Firstly start by ABCD for all traumatic pt. In HISTORY ;- # history of trauma or multi-traumatic pt. # Pain # vomiting # hematuria, hematochezia, # symptoms of hypovolemic shock
18 PHYSICAL EXAMINATION ;- # INSPECTION ;- Abrasions, Contusion, Laceration, Deformity # PALPATION ;-Tenderness, Rebound Tenderness Guarding # PERCUSSION ;- Dullness in hemoperitoneum, Subtle sign of peritonitis. # AUSCULTATION ;- Decrease bowel sound Factors compromising patient assessment Alcohol intoxication / use of illicit drugs Injury to the brain or spinal cord Injury to adjacent structures (ribs and spine).
19 Investigation Techniques - CBC, Liver function test, Serum Amylase, Urinalysis,, Blood type and crossmatch. - CXR and Plain X-ray of the abdomen - Ultrasound (FAST) - - Computer Tomography (CT SCAN) - - Diagnostic Peritoneal lavage(paracentesis) - Diagnostic laparoscopy
20 FAST Ultrasonography :(termed focused assessment with sonography in trauma [FAST]) can be done during the initial assessment (primary survey) without moving the patient to the radiology suite. The FAST images the pericardium, right and left upper quadrants, and pelvis; its primary aim is to find abnormal pericardial fluid or intraperitoneal free fluid. An extended FAST (E-FAST) adds images of the chest aimed at detecting pneumothorax.

21

22
23 CT is typically done with IV contrast: This test is very sensitive for free fluid and solid organ injury but less so for small viscus perforations and it can simultaneously detect injury to the spine or pelvis. Is there blood or peritoneal contamination?


24 DPL
25 * Laparoscopy: Types OF LAPAROSCOPY: Diagnostic laparoscopy Therapeutic laparoscopy In hemodynamically stable patients Inadequate/equivocal FAST or borderline DPL (80,000100,000 RBC/HPF) Intermittent mild hypotension or persistent tachycardia Persistent abdominal signs/symptoms Potential to decrease number of non-therapeutic laparotomies Avoids nontherapeutic laparotomies
26 Management blunt abdomen trauma
. Evisceration.")
27 Indications for laparotomy Following clinical evaluation, a few patients clearly require exploratory laparotomy rather than testing, including those with: Peritonitis. Hemodynamic instability due to penetrating abdominal trauma. Gunshot wounds (most). Evisceration. o
28 Complications: Delayed consequences of abdominal injury include:.hematoma rupture.intra-abdominal abscess.bowel obstruction or ileus.biliary leakage and/or biloma Abdominal compartment syndrome delayed incisional hernia
29 Penetrating abdominal injuries * Open wound in Abdominal. wall * Less common than blunt trauma * Caused by sharp object as knife or gunshot *The most commonly injured regions are the small bowel, large bowel, liver, and intra-abdominal vasculature

30

31
32 * Indications for exploration Local Wound Exploration Stab wounds that appear to be superficial should be explored under local anesthesia to determine if the parietal peritoneum was injured or not; if peritoneum found injured then laparotomy should be performed
33

34 Organs in abdomen trauma
35 SOLID ORGAN INJURY A- spleen Injury:- *The spleen is the most commonly injured organ in blunt abdominal trauma. The injury should be suspected when the 9-10th ribs on the left are fractured, or when left upper quadrant tenderness and tachycardia are present. Commonly the patient complains of pain in the left shoulder but this is usually not present for an hour or two. Peritoneal signs such as rebound sensitivity and guarding will be delayed until the blood has had time to cause local irritation of the peritoneum. Any patient with tachycardia or hypotension and left upper quadrant tenderness is assumed to have a ruptured spleen until proven otherwise. Establish the diagnosis by Abdomen U/S in patients with evidence of significant hemorrhage, or by CT scanning in those who are stable.


36 Splenic injury grading by CT scan to 5 grade by American Association for the Surgery of Trauma

37
38 TREATMENT * Non-operative treatment Criteria of non-operative treatment: 1) The patient should be hemodynamically stable. 2) Negative abdominal examination. 3) Absence of contrast extravasation on CT-scan. 4) Absence of other clear indications for exploratory 5) Grade 1& 2 6) The operating room facilities and personnel are available in the event of sudden bleeding that requires splenectomy
39 1-Patients are admitted to I.C.U. for hours, for monitoring of vital signs, serial physical examination, serial hematocrit and abdomen U/S. 2- I.V Fluid, analgesic, antibiotic Blood Transfusion if need - 4- Observe in hospital for days, bed rest for 1 week - 5- No strenuous activity for 6-8 weeks 6- No contact sports for 6 months. - - NOTE: delayed Splenic hematoma rupture and hemorrhage may occur. Usually in two days to two weeks nonoperative management of children with splenic injury. - splenectomy avoided in >90% of children and 50% - 60% of adults by non operative management.
40 Operative Treatment ;- * Splenorrhaphy ;- * Splenectomy ;- is usually indicated under the following circumstances: 1- The patient is unstable 2-The spleen is extensively injured with continuous bleeding, splenic avulsion, fragmentation or rupture, extensive hilar injuries. 3- Other injuries require prompt attention as peritoneal contamination from GI injury. Note: Polyvalent pneumococcal vaccine should be given after splenectomy


41 B- Liver Injury * The liver may be lacerated by either blunt or penetrating trauma. * Second most commonly injured after blunt abdominal trauma. * Diagnosis by CT in stable patients and by laparotomy in unstable patients
42 Liver injury Clinical Findings Suspect liver laceration when blunt trauma or penetrating trauma involves the right lower chest or right upper abdomen, or when right upper quadrant pain, tenderness, fractures of the 7-9th ribs overlying the liver. Rebound and guarding will not be present until blood has been in the abdomen long enough to cause peritoneal irritation about two hours..

43


44 Liver injury grading by CT scan to 6 grade by American Association for the Surgery of Trauma
45 TREATMENT * Non-operative treatment ; Criteria of non-operative a) Blunt injuries in hemodynamically stable patients b) Low grade liver injury (I to III). c) Transfusion need of less than 2 units of blood. d) Stable patients with Absence of peritoneal signs. e)no extravasation in CT scan with contrast. * Treatment ;- 1-Patients are admitted to I.C.U. for monitoring of vital signs and serial hematocrit for hours. 2- Bed rest for 5 days. 3- Resumption of normal physical activity after 3 months post-injury
46 Operative Indicated under the following circumstances: 1- The patient is unstable. 2-Other injuries require prompt attention; 3-The Liver is extensively injured with continuous bleeding. 4-Bleeding is associated with hilar injury. Injuries of the liver require ;- (( obtaining good hemostasis, remove of dead tissues, adequate drainage, Prehepatic packing, pringle maneuver and damage control surgery)).

47 C- Pancreatic injury Most common after blunt abdomen trauma, Most often due to direct epigastric blow compressing pancreas against vertebral column, often associated with duodenal, hepatic and splenic trauma. also occurs in association with lower thoracic or upper lumbar vertebral fracture. The patient often experiences vague upper and mid-abdominal pain that radiates into the back. Helical abdominal CT most useful investigation. ERCP (endoscopic retrograde cholingo pancreatic) Subsequent rise in amylase can helpful.
48 Grades I and II include minor pancreatic contusions and lacerations that spare the pancreatic duct. Grade III injuries include pancreatic duct injuries at the body and tail. Grade IV injuries include ductal injuries at the pancreatic head. Grade V injuries include massive disruption of the pancreatic head. Management: (a) Simple injury without involvement of the pancreatic duct needs only drainage (b) Injuries of the pancreatic duct distal to the head can be managed by distal pancreatectomy (c) In severe injuries of the head with severe associated duodenal injuries pancreatico-duodenectomy (Whipple s operation) is used rarely as it carries high mortality

49 HOLLOW ORGAN INJURY 1- STOMACH INJURY: Stomach rupture causes rapid onset of burning epigastric pain, followed quickly by rigidity and rebound sensitivity # Minor injuries can be debridement and primary repair with simple suture closure. # Larger injuries can be resected and primary repair. (1
50 2) Duodenum: Injuries to the duodenum are graded as follows: (I) hematoma; (II) partial thickness laceration; (III) laceration disrupting 75% circumference of D2, or involving the ampulla or distal common bile duct; and (V) massive disruption of the duodenopancreatic complex or devascularization of the duodenum. Management: (a) Small injuries kocherization of the duodenum and primary repair of the tear. (b) Larger tears are anastomosed by Roux-en-Y technique, or Repair and combined with diversion of food by gastro-jejunostomy or duodenal exclusion.

51 4) Small intestine: a- Minor injuries can be repaired by simple suture closure in transverse direction, b-multiple injuries localized near to each other and larger injuries need resection of that part and primary anastomosis
52 5- Colon:- Management: (a) Small injuries with minimal associated injuries in stable patients can be debridement and primary repair. (b) Unstable patients or patients with multiple associated injuries will require colostomy following resection of the injured part (c) Cecal injuries cecal repair or resection and anastomosis. (d) Larger injuries to the right colon with minimal associated injuries can be debridement and primary repair, resection and primary anastomosis (right hemicolectomy).
53 (e) Larger injuries of the transverse colon can be primary repair, resection and anastomosis or transformed to colostomy. (f) Injuries of the splenic flexure and descending colon primary repair, resection and anastomosis with or with out protective proximal colostomy or transformed to colostomy (g) Large injuries of the sigmoid - after resection of the injured part, either Hartmann s colostomy or double-barrel colostomy is performed 6-Rectum: Injuries to the rectum will require repair of the injured part, proximal diverting colostomy, and presacral drainage
54 Diaphragmatic injury Diaphragmatic injury more with penetrating trauma but <5% of cases with blunt trauma, left sided in 80% of cases. suspect with penetrating injury below 5th rib, diagnosis may be difficult, but CT, MRI can be help. Laparoscopy provides good views of diaphragm. spontaneous healing does not occur injuries should be repaired either via laparotomy or with laparoscopic or thoracoscopic techniques.
55 RETROPERITONEA HEMATOMA ( it is defined as bleeding into retroperitoneal space ) * Source: aorta, IVC, kidneys and ureters, pancreas, pelvic fracture, retroperitoneal bowel. * Minimal signs on examination; flank pain and contusion are late findings * FAST/DPL negative; CT can identify.


56 GREY TURNER SIGN CULLEN S SIGN

57 * The Retroperitoneum can be divided into three anatomic zones for purposes of decision making..
58 * Central retroperitoneal hematomas (Zone-1) :- Are associated with pancreaticoduodenal injuries or major abdominal vascular injury. * Flank or perinephric hematomas (Zone-2):- May be associated with injuries to the genitourinary tract or, in the case of penetrating trauma, with injuries to the colon. * Zone-3 injuries:- Which are confined to or originate from the pelvis, are most often associated with pelvic fractures



59
60 * Retroperitoneal hematomas in Zone-1, regardless of cause or size, are formally explored * Zone-2 hematomas caused by penetrating injuries should routinely be explored. * Zone-2 hematomas caused by blunt trauma can be left alone if they are not expanding and not pulsating and the intravenous urogram is normal * Zone-3 retroperitoneal hematomas in patients with penetrating injuries are usually explored to exclude major vascular injuries. Local bleeding encountered at exploration under these circumstances is usually easy to control, and the associated injuries can be identified. * Patients with Zone-3 hematomas secondary to blunt trauma usually have associated pelvic fractures. Exploration of the hematoma can be hazardous and is usually avoided
61 CONSERVATIVE TREATMENT OF RETROPERITONEAL HEMATOMA Complete bed rest Pain killers Appropriate amount of blood replacement I.V. fluids in high amounts. I.V. Sodium bicarbonate prevents precipitation of hemoglobin in renal tubules In the absence of hypovolemia and after infusion of large amounts of I.V. fluids LASIX should be given to enforce diuresis High doses of broad spectrum antibiotics, follow-up and observation of vital signs and diuresis
62 Renal and Urinary tract injury Kidney injury: is more common after blunt trauma like falls and automobile accidents. Suspect it with fractures of the 11th- 12th ribs, flank tenderness or hematuria Kidney lacerations can bleed extensively into the retroperitoneal space. CT is examination of choice if hemodynamically stable. IVP can be use. Majority of renal injuries can be treated conservatively, Surgical intervention is mandatory for any kidney that shows extravasation of dye.
63 Urinary Bladder injury: Rupture commonly associated with pelvic fractures, >95% hematuria, Retrograde cystography is investigation of choice. Management: Intraperitoneal rupture requires operative repair while extraperitoneal rupture can be treated conservatively. Urethral trauma: Should be suspected if there is blood at meatus, perineal injury or abnormal position of prostate. Management: is suprapubic drainage and delayed definitive repair
64 Pelvic injury Associated with a mortality of 13-23% and significant morbidity. In majority of patients massive retroperitoneal hemorrhage is direct cause or a major contributing factor to mortality Mechanism of injury: Significant pelvic fractures are due to high energy blunt trauma. Usually a RTA, fall or crush injury. Pelvic injury Clinical features: -suggested by pain on movement, structural instability, gross hematuria, peri pelvic ecchymoses -rectal examination mandatory to identify rectal injury and prostatic position -if patient has a stable pelvic fracture hypotension is probably due to hemoperitoneum



65
66 Complications of comminuted fracture of the pelvis: Acute: major hemorrhage (leading cause of death) shock elevated intra- abdominal pressure. visceral and soft tissue injury: fractures may be compound into the perineum or vagina, or be associated with lacerations into the rectum or bladder (esp. with lateral compression and vertically unstable injuries). urethral injuries common in males. insertion of a urethral urinary catheter contraindicated sacral plexus injury ileus pain fat embolization acute respiratory distress syndrome: in about 15%. This is possibly related to the frequent occurrence of associated thoracic injuries, multiple blood transfusions, shock, and fat embolization. DVT because of stasis resulting from prolonged bed rest, and prophylaxis is often contraindicated Late: infection-second most common cause of death disability/immobility/instability incontinence pain

67 Pelvic injury Management: Initial management: --ABC, I.V Fluid, Analgesic --Pelvic wrap or Binder -- Foleys catheter insertion but contraindicated if urethral injury suspected --Blood transfusion if need
68 Pelvic injury Management: bleeding is usually bony or venous in origin if patient is still hemodynamically unstable perform early FAST OR open DPL. If grossly positive laparotomy should precede external fixation or angiography. If NEGETIVE control of pelvic bleeding becomes main priority early stabilization with external fixators helps to minimize bleeding from veins and small arterioles near fracture sites, pelvic angiography with embolization often successful in controlling Small arterial hemorrhage but large vessel bleeding requires surgical control preperitoneal packing, early operative stabilization of complex pelvic fractures preferred. ICU: facilitates respiratory care, pain control and early mobilization. compound fractures involving perineum, rectum or vagina require aggressive surgery to avoid high mortality

69
70 Thank You